Most people know that mixing two pills can cause problems. But what if your health condition itself makes a medication dangerous-even if you’re taking it exactly as prescribed? This is the hidden risk of drug-disease interactions. It’s not about pills clashing with each other. It’s about how your body’s existing illnesses change how a drug behaves. And it’s happening more often than you think.
What Exactly Is a Drug-Disease Interaction?
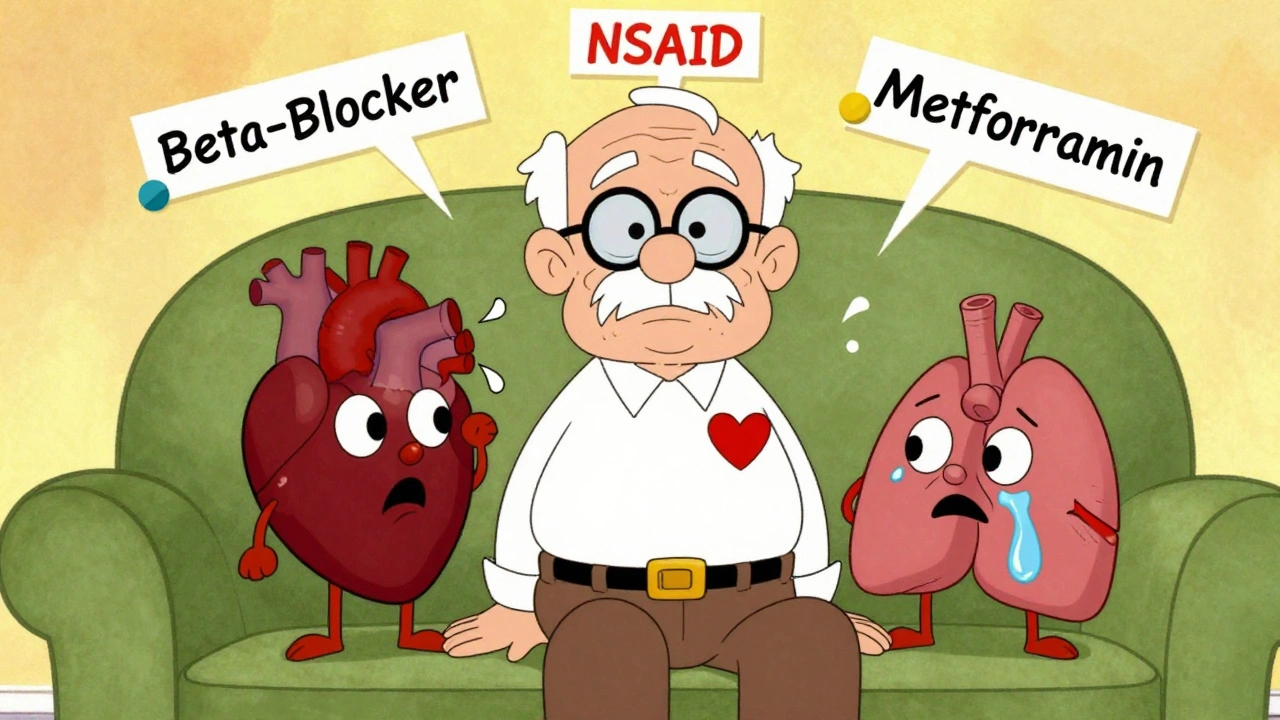
A drug-disease interaction (also called a drug-condition interaction) happens when a medication meant to treat one health problem makes another condition worse-or stops working properly. For example, a beta-blocker for high blood pressure might hide the warning signs of low blood sugar in someone with diabetes. Or an NSAID for arthritis could cause fluid buildup and make heart failure worse. These aren’t side effects you can predict from the label. They’re hidden risks tied to your unique health profile.The problem is growing. The average American over 65 takes five or more medications. And nearly half of them have three or more chronic conditions. That means more chances for a drug to accidentally harm another part of your body. The Agency for Healthcare Research and Quality estimates that 5 to 10% of hospital admissions are caused by medication problems-and many of those come from undetected drug-disease interactions.
How Do These Interactions Actually Happen?
There are five main ways your health condition can interfere with a drug:- Pharmacodynamic interference: The drug’s effect fights against your disease. Beta-blockers reduce heart rate, but in someone with asthma, they can tighten airways and trigger an attack.
- Pharmacokinetic changes: Your disease alters how your body processes the drug. Liver disease slows down the breakdown of warfarin, making it too strong and raising bleeding risk.
- Masking symptoms: The drug hides warning signs. Beta-blockers can stop you from feeling your heart race during low blood sugar, so you don’t know to eat something until it’s too late.
- Exacerbating complications: The drug worsens the side effects of your condition. NSAIDs cause your body to hold onto salt and water, which increases pressure on a weakened heart in heart failure patients.
- Direct organ toxicity: The drug damages an organ already struggling. Metformin, a common diabetes drug, can cause lactic acidosis in people with kidney disease because their kidneys can’t clear it.
Some conditions are far more likely to cause these problems. Chronic kidney disease, heart failure, liver disease, and psychiatric disorders like depression account for nearly 80% of serious drug-disease interactions. For example, in patients with depression, antidepressants like SSRIs can increase bleeding risk-especially if they’re also taking blood thinners. In heart failure, certain diabetes drugs like SGLT2 inhibitors can raise the risk of diabetic ketoacidosis, especially if kidney function is already poor.
Why Are These Interactions So Often Missed?
You’d think doctors and pharmacists would catch these. But they don’t always. A 2020 review found that only 16% of clinical guidelines for common conditions like diabetes, depression, or heart failure include clear warnings about drug-disease interactions. Most guidelines focus on treating one disease at a time, not how treatments affect the whole patient.Electronic health records are supposed to help. Systems like Epic flag up to 87% of high-risk interactions. But they also generate false alarms 42% of the time. Doctors start ignoring them. That’s called alert fatigue. By the time a real danger pops up, the system’s been drowned out by noise.
Even pharmacists struggle. A 2021 survey found that community pharmacists spend an average of 12.7 minutes per patient just checking for drug-disease risks. But most dispensing appointments last less than five minutes. There’s just not enough time.
Patients aren’t better off. A survey from Village Medical found only 22% of people with high blood pressure knew why decongestants like pseudoephedrine could spike their blood pressure. Yet 89% of them had been prescribed these over-the-counter cold medicines. If patients don’t know the risks, they won’t ask questions.

Who’s Most at Risk?
Older adults are the most vulnerable. The FDA reports that people over 65 average 5.4 medications and 4.7 chronic conditions. That’s a perfect storm for interactions. The 2023 update to the Beers Criteria-the gold standard for unsafe medications in seniors-added 12 new drug-disease warnings. Now it specifically warns against anticholinergics in dementia patients (they speed up cognitive decline) and opioids in people with COPD (they can suppress breathing).But it’s not just age. People with limited access to care are at higher risk too. A 2023 study in Health Affairs found that marginalized groups-Black, Hispanic, and low-income patients-experience 23% more drug-disease-related hospitalizations. Why? Fragmented care. Multiple doctors. No one pulling the full picture together.
What Can You Do to Protect Yourself?
You don’t have to wait for the system to fix itself. Here’s what works:- Keep a full, updated list of everything you take. That includes prescriptions, over-the-counter meds, vitamins, supplements, and herbal products. St. John’s wort, for example, can cause life-threatening serotonin syndrome when mixed with SSRIs. Many people don’t realize it’s a drug.
- Ask your pharmacist or doctor: “Could any of these meds make my other conditions worse?” Don’t wait for them to bring it up. Be specific. Say: “I have kidney disease-could this new pill hurt my kidneys?”
- Know the red flags. If you start feeling worse after a new medication-dizziness, swelling, confusion, sudden fatigue, or irregular heartbeat-call your provider. Don’t assume it’s just “part of aging.”
- Get regular medication reviews. Every six months, ask for a full med check. Focus on kidney and liver function. These organs handle most drugs. If they’re not working well, your meds can build up to dangerous levels.
- Use the DUP-OP-ALT framework. Ask: Is this drug Duplicating another? Is it OPposing my condition? Is it ALTering how another drug works? This simple checklist helps you spot risks before they become problems.
What’s Changing in the Medical World?
There’s progress. The FDA now requires drug makers to test how their medications affect patients with common comorbidities-not just healthy volunteers. The European Medicines Agency has made drug-disease interaction sections mandatory in all new drug applications. And the NIH’s All of Us program is using AI and genetic data to predict individual risks with 38% more accuracy than before.Some hospitals are seeing real results. Mayo Clinic’s DDSI screening program cut medication-related readmissions by 27% in just two years. The Centers for Medicare & Medicaid Services now penalizes hospitals with high rates of drug-related harm. That’s forcing change.
But the system still isn’t catching most of these interactions. That’s why your role matters. You’re the one who knows your body best. You’re the one who notices when something feels off. Don’t let the complexity of modern medicine make you passive.
What About Supplements and Herbal Products?
They’re not safer. In fact, they’re riskier. St. John’s wort, ginkgo biloba, garlic supplements, and even high-dose vitamin E can interfere with prescription drugs. They’re not regulated like medications, so their strength and effects vary wildly. And most doctors don’t ask about them. You have to volunteer the information.For example, ginkgo can increase bleeding risk if you’re on warfarin. Garlic can lower blood pressure too much if you’re already on antihypertensives. And St. John’s wort can trigger serotonin syndrome with antidepressants. These aren’t myths. They’re documented, life-threatening risks.
Final Thought: Your Health Is a System-Not a List of Problems
Treating high blood pressure, diabetes, and arthritis as separate issues is outdated. Your body doesn’t work that way. A drug that helps one part can hurt another. And the more conditions you have, the more carefully you need to watch what you take.The goal isn’t to avoid medicine. It’s to use it wisely. The right drug, at the right dose, for the right person-considering every part of their health-is what saves lives. You can’t wait for your doctor to figure it all out. Be informed. Be vocal. Be your own best advocate.
Can a drug-disease interaction happen even if I take my meds exactly as prescribed?
Yes. Drug-disease interactions aren’t about taking too much or mixing pills incorrectly. They happen because your body’s existing condition changes how the drug works. For example, someone with kidney disease might take metformin exactly as directed, but their kidneys can’t clear it properly-leading to dangerous lactic acidosis. The dose is right, but the condition makes it unsafe.
Which health conditions are most likely to cause dangerous drug interactions?
Chronic kidney disease, heart failure, liver disease, and psychiatric conditions like depression are the top four. Together, they account for about 78% of serious drug-disease interactions. Kidney and liver problems affect how drugs are processed. Heart failure is sensitive to fluid balance and blood pressure changes. Depression treatments carry bleeding and toxicity risks, especially when combined with other meds.
Are over-the-counter drugs safe if I have multiple health conditions?
Not always. Common OTC meds like NSAIDs (ibuprofen, naproxen), decongestants (pseudoephedrine), and antacids can cause serious problems. NSAIDs worsen heart failure and kidney disease. Decongestants raise blood pressure and can trigger heart rhythm issues. Even antacids can interfere with absorption of other medications. Always check with your pharmacist before taking anything new.
Why don’t my doctors warn me about these interactions?
Many clinical guidelines still focus on treating single diseases, not whole patients. Only 16% of guidelines for common conditions like diabetes or heart failure include clear warnings about drug-disease risks. Doctors are under time pressure, and electronic systems flood them with false alerts. It’s not negligence-it’s a broken system. That’s why you need to ask questions.
How can I tell if a new medication is causing a drug-disease interaction?
Watch for new or worsening symptoms after starting a drug. For example: swelling in your legs (could mean heart failure is worsening), confusion or dizziness (could be a drug building up in your system), or sudden low blood sugar without warning (could mean a beta-blocker is masking symptoms). If something feels off, don’t ignore it. Write down what changed and when-and call your provider.
Is there a tool or checklist I can use at home to check for risks?
Yes. Use the DUP-OP-ALT framework: Ask if the new drug is Duplicating another (two drugs doing the same thing), OPposing your condition (fighting against your disease), or ALTering another drug’s effect (changing how something else works). Also, use the Beers Criteria for older adults-it’s free online and lists unsafe drugs for common conditions. Keep your med list updated and review it every six months.
 Tizanidine and Ciprofloxacin Interaction: Risks of Severe Hypotension and Sedation
Tizanidine and Ciprofloxacin Interaction: Risks of Severe Hypotension and Sedation
 Efavirenz and Blood Pressure: Essential Facts and Management Tips
Efavirenz and Blood Pressure: Essential Facts and Management Tips
 Food Environment: How to Set Up Your Home Kitchen to Support Weight Loss Goals
Food Environment: How to Set Up Your Home Kitchen to Support Weight Loss Goals
 Hemophilia and Alcohol: Essential Facts and Safe Practices
Hemophilia and Alcohol: Essential Facts and Safe Practices
 Why American Mistletoe is the Perfect Addition to Your Daily Supplement Routine
Why American Mistletoe is the Perfect Addition to Your Daily Supplement Routine
Declan O Reilly
December 3, 2025 AT 01:49Man, this hit me right in the feels. I’ve been on 7 meds for years and never thought about how my kidney issues might be turning my diabetes drug into a ticking time bomb. Thanks for laying it out like this - it’s not just about popping pills, it’s about your whole damn body being one messy, interconnected machine.
My grandma died because no one checked if her heart meds were making her liver fail. We thought it was just ‘old age.’ It wasn’t. It was negligence wrapped in a white coat.
Conor Forde
December 4, 2025 AT 11:33Oh here we go. Another ‘you’re all gonna die from your own meds’ panic essay. Newsflash: if you’re taking 5+ pills, you’re probably already a walking clinical trial. The real problem? Pharma doesn’t want you to know how many of these drugs were tested on 22-year-old college kids with zero comorbidities. That’s not science - that’s corporate laziness.
Also, ‘St. John’s Wort is dangerous’? DUH. It’s a plant. Plants don’t come with FDA warning labels because they can’t afford lawyers. But hey, let’s blame the patient for not knowing Latin pharmacology terms, right?
patrick sui
December 6, 2025 AT 08:02Really appreciate this breakdown 🙏. The DUP-OP-ALT framework is gold - I’ve started using it with my dad who’s got CHF + diabetes + depression. He didn’t realize his OTC sleep aid was an anticholinergic. Now he’s off it and sleeping better without the brain fog.
Also, the 12.7 min pharmacist stat broke my heart. We’re asking humans to do quantum physics in 5 minutes while juggling 30 other patients. No wonder mistakes happen. We need systemic change - not just ‘be more careful’ advice.
And yes, supplements are wild west. Ginkgo + warfarin = bleeding risk. Garlic + BP meds = fainting in the grocery aisle. These aren’t myths. They’re documented. Please tell your auntie she can’t ‘boost immunity’ with 10 pills a day.
Priyam Tomar
December 7, 2025 AT 17:52Typical western medical nonsense. In India, we’ve been treating patients with multiple chronic conditions for decades without all this overcomplicated jargon. We use fewer drugs. We rely on diet, fasting, and Ayurveda. Your system is broken because you over-medicalize everything.
Metformin causes lactic acidosis? So stop giving it to kidney patients. Simple. No need for 10-page essays. Also, why are you trusting American guidelines? They’re funded by Big Pharma. Check Chinese or Indian clinical data - they’re more realistic.
Jack Arscott
December 9, 2025 AT 17:22Y’all need to chill. I’m 72, have 4 conditions, take 6 meds, and I’m still hiking every weekend 😎
Just talk to your doctor. That’s it. No need to overthink it. Also, I use St. John’s wort for my mood and it’s been fine for 8 years. Maybe my body’s just built different 🤷♂️
Irving Steinberg
December 10, 2025 AT 02:02So basically the system is broken and we’re all just supposed to become pharmacists on top of having jobs and families and kids and life?
Great. Just great. I’m tired. I just want to take my pill and not have to memorize the pharmacokinetics of every damn thing I put in my mouth. If my doctor can’t keep track, why should I?
Also I hate when people say ‘be your own advocate’ like it’s a motivational poster. I’m not a lawyer. I’m a human who’s tired.
Also I think ginkgo is fine. I’ve been taking it since 2015 and I haven’t bled out yet 🤷♂️
Lydia Zhang
December 10, 2025 AT 13:54Interesting. I take five meds. I have three conditions. Never thought about this. Will ask my pharmacist next time. Maybe.
Also I don’t know what DUP-OP-ALT means. Too many letters.
Kay Lam
December 10, 2025 AT 15:00One thing I’ve noticed after working in geriatric care for over 20 years is that the most dangerous interactions aren’t always the ones flagged by the system - they’re the ones that sneak in quietly, like a slow leak in a pipe you didn’t know was cracked. A patient on lisinopril for hypertension gets prescribed an NSAID for arthritis pain, and over three months their creatinine slowly climbs, their potassium spikes, they get dizzy, and no one connects the dots because each visit is focused on one issue - the arthritis, then the dizziness, then the lab result - never the whole picture. It’s not that anyone’s negligent, it’s that the system is designed in silos. We treat hypertension, we treat arthritis, we treat depression - but we rarely treat the person who has all three at once. And that’s where the real harm happens. You can’t fix a system that refuses to see the whole human. You have to be the one to ask: ‘What else is going on?’
And yes, your ‘natural’ supplements? They’re not natural to your liver. They’re chemicals. And your body doesn’t care if they’re from a plant or a lab - it just tries to process them. And if it’s already stressed from heart failure or kidney disease? It’s not equipped for the extra load. So when your cousin says ‘I take turmeric for inflammation,’ ask her if she’s on warfarin. And if she says ‘no,’ ask again. Because she might not know.
Matt Dean
December 10, 2025 AT 16:19Let’s be real - if you’re over 65 and on five meds, you’re basically a walking FDA case study. You’re not a patient, you’re a liability. The system isn’t designed for people like you. It’s designed for healthy people who take one pill for one thing. So stop pretending you’re entitled to all these drugs. You’re lucky you’re not on dialysis already.
Also, ‘St. John’s wort is dangerous’? Shocking. Who knew plants could interact with chemicals? Next you’ll tell me water can drown people.
Walker Alvey
December 12, 2025 AT 13:19Oh wow. Someone finally admitted the truth: doctors are just overworked clerks with stethoscopes. And we’re supposed to trust them with our lives? Brilliant. Let’s just add ‘medication roulette’ to the list of American pastimes along with Obamacare and student loans.
Also, ‘DUP-OP-ALT’? That’s not a framework, that’s a corporate buzzword salad. You could’ve just said ‘think before you swallow.’ But no, we need 5-letter acronyms to feel smart.
And yes, I know someone who died from this. No one told her the beta-blocker was hiding her hypoglycemia. She passed out in her kitchen. They found her 12 hours later. The chart said ‘no drug interactions.’
System failure. Not patient failure.
Adrian Barnes
December 14, 2025 AT 05:53This article is a textbook example of emotional manipulation disguised as medical education. The data is cherry-picked to induce fear, the tone is deliberately alarmist, and the solutions are vague platitudes wrapped in pseudo-scientific jargon. The fact that you’ve reduced complex polypharmacy to a checklist implies a fundamental misunderstanding of clinical decision-making. The Beers Criteria is not a Bible - it’s a guideline with significant limitations, particularly in diverse populations. Furthermore, your conflation of pharmacokinetic variability with patient negligence is ethically indefensible. The burden of cognitive labor should not fall on the elderly, the economically disenfranchised, or the medically underserved. The onus lies squarely on institutions that refuse to invest in integrated care models, interoperable EHRs, and clinical pharmacists embedded in primary care teams. Until then, your ‘DUP-OP-ALT’ framework is a Band-Aid on a hemorrhage.
Michelle Smyth
December 15, 2025 AT 11:58How quaint. Another American think-piece about how ‘the system’ is broken. In Europe, we’ve had integrated care pathways for decades. We don’t need a checklist called DUP-OP-ALT - we have multidisciplinary teams. We don’t rely on overworked pharmacists to catch errors in five minutes - we have clinical pharmacists embedded in GP practices. And we don’t treat patients like they’re supposed to be amateur pharmacologists. We treat them like people. But of course, you Americans need another blog post to feel like you’re doing something. Meanwhile, your life expectancy is falling and your healthcare costs are skyrocketing. How’s that ‘advocacy’ working out for you?
Linda Migdal
December 15, 2025 AT 14:04Look, I get it. But this isn’t about ‘drug-disease interactions’ - it’s about American healthcare being a profit-driven dumpster fire. We don’t have a system, we have a marketplace. You want to fix this? Stop letting insurance companies dictate what drugs get approved. Stop letting pharma fund clinical trials. Stop letting doctors get paid per script. Then maybe, just maybe, we’ll stop treating patients like walking pharmacies.
Also, St. John’s wort? It’s been used for centuries. Your ‘science’ is just corporate branding with a lab coat.
Tommy Walton
December 15, 2025 AT 14:33So basically: your body’s a minefield and your doctor’s asleep? Cool. I’ll just keep taking my pills and hoping for the best 🤷♂️
Also I love how they say ‘ask your pharmacist’ - like they have 47 minutes to talk to me. 😂
James Steele
December 16, 2025 AT 18:15It’s not just about drug-disease interactions - it’s about the epistemological collapse of medical authority. We’ve outsourced clinical judgment to algorithmic decision trees and EHR pop-ups that are statistically noise-laden. The Beers Criteria? A heuristic artifact of an aging population, not a biological truth. And the DUP-OP-ALT framework? A linguistic shell game to make patients feel empowered while the real structural failures - underfunded primary care, fragmented records, lack of pharmacogenomic integration - remain untouched.
The real issue isn’t that patients don’t know their meds. It’s that the system refuses to acknowledge that human physiology is not modular. You can’t treat diabetes, depression, and heart failure as separate entities. You’re treating a single organism with a thousand variables - and you’re doing it with a checklist. That’s not medicine. That’s bureaucracy with a stethoscope.
Declan O Reilly
December 17, 2025 AT 01:40Replying to @patrick sui - you’re right about the pharmacist time crunch. I asked mine last week and she literally said, ‘I have 12 patients waiting, I’ll flag this one.’ I felt like a burden. But then she added, ‘Wait - you’re on metformin and have CKD? Let me call your doctor right now.’
That’s the moment it changed. Not the checklist. Not the article. Just one human who paused.
Maybe the solution isn’t more tools. Maybe it’s more time. More care. More humanity.